





Improving Management of Pain Associated With Intrauterine Device Insertion
In the United States, almost half (45%) of all pregnancies among adolescents and women aged 15 to 44 years from 2008 to 2011 were unplanned.1 This percentage represents a decline from the last assessment by the National Center for Health Statistics in 2008. The decline likely was due to an overall increase in use of contraceptives—especially long-acting reversable contraceptives (LARCs) such as intrauterine devices (IUDs)—by adolescents and women at risk of unplanned pregnancy over this time period.1 However, unintended pregnancies were more common among women with lower incomes and lower levels of education.1 Some racial and ethnic disparities have narrowed in recent years, yet disadvantaged Black and Hispanic women have higher rates of unplanned pregnancies than do White women and those having higher incomes.1
LARCs such as IUDs have greater rates of efficacy, length of continuation, and patient satisfaction than do short-acting contraceptives.2 For contraception among sexually active young women and adolescents, the levonorgestrel-releasing intrauterine system (LNG-IUS) and the copper-containing IUD (Cu-IUD) are endorsed by the American College of Obstetricians and Gynecologists, the Society of Obstetricians and Gynecologists of Canada, and the European Society of Contraception and Reproductive Health.3 Their use is also supported by the North American Society for Pediatric and Adolescent Gynecology and the American Academy of Family Physicians.4,5 In addition to contraception, the LNG-IUS offers noncontraceptive benefits (eg, treatment for dysmenorrhea, endometriosis, or heavy menstrual bleeding).6
When properly used, the LNG-IUS and the Cu-IUD are associated with 0.2% and 0.6% failure rates overall, respectively, which are comparable to rates noted with tubal sterilization (0.5%).2,7 By contrast, oral contraceptives, which are used more frequently by young women and adolescents, are 20 times less effective than are IUDs.8,9
Yet, despite their endorsements by professional societies and groups and records of safety and efficacy, IUDs continue to have a low uptake by adolescents and young women.3-5,8 Among US adolescents who used contraceptives between 2011 and 2015, only 2.8% used an IUD.2 The underuse of IUDs may be attributed to anxiety related to IUD placement and fear of pain associated with the procedure.2,6
PATIENT-REPORTED PAIN VERSUS PHYSICIAN-PERCEIVED PAIN
Physicians tend to underestimate patients’ pain levels.10 Accurate pain assessment is critical for recognition, choice of the best analgesic, and determination of patient response to a particular analgesic method. Pain is often determined using either the numerical rating scale (with zero on a 10-cm scale indicating no pain and 10 representing the worst pain) or a visual analog scale (VAS).10,11 The VAS score is a validated standard instrument for assessing pain in clinical research; similar to the numerical rating scale, a score of zero indicates no pain and a score of 10 represents the worst pain imaginable.11

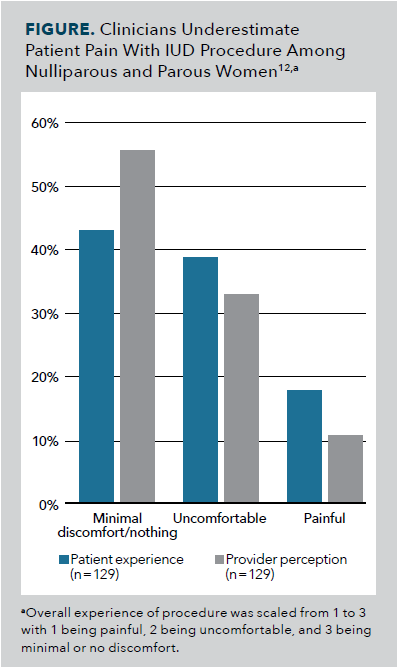
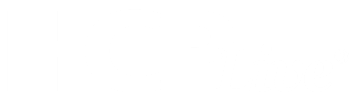
Pain is naturally subjective and influenced by personal experience. Those factors alone make it difficult for someone to assess another person’s pain; however, a physician’s perception of patients’ pain can be compounded by numerous additional factors, including professional experience, personality, communication style, and clinical environment.10 Survey results from 284 women showed that patients’ pain level associated with IUD insertion was higher than that observed by their clinicians (Figure).12 These results highlight the need to educate physicians about improving their assessment of and response to patients’ pain.
With IUD insertion, most women experience a sensation similar to that of menstruation discomfort, but some experience moderate to severe pain.13,14 VAS pain scores on a 10-mm line related to IUD insertion have ranged from 2 to 7.15 This pain may be related to several aspects of the insertion process, including placement of the tenaculum (a type of forceps), use of the uterine sound, insertion of the IUD in the cervix, and contact with the uterine fundus.16
Women who have not given birth generally report considerably more pain with IUD insertion than do those who have borne children, although the procedure does not vary between these populations.2,12,17 Women with dysmenorrhea or anxiety may also experience greater pain.18 Additional aspects related to anatomy, psychology, and culture may also contribute to discomfort.19
The discrepancy between provider and patient perception can apply specifically to the pain associated with IUD insertion.10,12 Patients often do not receive pain management for the procedure; the decision to receive analgesia largely is based upon the preference of the provider and counseling given to the patient.15 Notably, patients have indicated willingness to undergo certain inconveniences (eg, applying topical pain therapies, extending visit time in the clinic) to better control pain.16
It is important for clinicians to be aware of the potential for pain, recognize that it is an important issue for patients, and familiarize themselves with pain management options. This awareness may enable clinicians to optimally educate patients, support their relaxation and comfort with the procedure, and select appropriate pain management as needed.12
PAIN MANAGEMENT STRATEGIES FOR IUD INSERTION
Currently, there are no official guidelines or standards of care for managing pain associated with IUD insertion.16 Comparison of pain management strategies used in clinical studies may be challenging because of variations across patient groups, randomization procedures, types of IUDs used, pain assessment protocols, and analgesia approach. In addition, many women experience no or minimal pain without any pain management, which complicates understanding of how analgesia affects the patient experience.19
Results from a 2015 Cochrane review indicated that use of certain oral analgesics and forms of lidocaine helped to reduce pain during IUD insertion among some patient groups.20 Authors of a 2019 literature review noted that findings from that Cochrane review primarily were culled from single, moderate-quality studies; the outcomes of the 2019 review similarly showed that use of various lidocaine preparations before IUD insertion was associated with clinically relevant positive effects on patients’ experience of insertion pain. However, the authors stated that the routine use of lidocaine continues as a point of discussion.19
Oral analgesia
Over-the-counter (OTC) oral analgesia allows patients to take the medication before having the procedure and provides time savings and affordability. In this context, use of nonsteroidal anti-inflammatory drugs (NSAIDs) has been studied the most.13 Ibuprofen has been used in randomized trials, but this common NSAID has not been associated with less IUD insertion pain.13 The NSAID ketorolac, by contrast, may offer overall pain relief. In 1 study, ketorolac, 20 mg, or placebo was given by mouth 40 or 60 minutes prior to IUD insertion.21 Patients who received ketorolac experienced improved pain reduction during the procedure, 10 minutes after the procedure, and overall when compared with the placebo group.21 The greatest analgesic effect obtained with oral ketorolac most likely occurs 1 to 2 hours following administration; therefore, this pain management strategy may not be applicable in outpatient settings. Use of oral ketorolac, 20 mg, for an IUD procedure may be feasible for eligible patients if it is prescribed with instructions to consume 1 hour before the appointment.21
Use of the NSAID naproxen sodium to manage the pain of IUD insertion has also been studied. Outcomes from a study regarding naproxen sodium, 550 mg, given by mouth 60 minutes before IUD insertion showed that use of this agent did not reduce pain during insertion. It did, however, result in less pain after the procedure.13 To support pain reduction following the procedure, clinicians could recommend that patients take two 220-mg naproxen sodium tablets (OTC strength) before their arrival. Clinics may also offer 550-mg tablets (prescription strength) on-site for patients who are not able to take the medication prior to the appointment.13
With consideration of these study outcomes, certain NSAIDS (ketorolac and naproxen sodium) may offer notable analgesic effects during and following the IUD procedure.13,21
Local analgesia
Use of local analgesia involving lidocaine formulations delivered via paracervical blocks, creams, and self-administered gels has also been explored.8,16,22-24 The lidocaine gels, evaluated as preparations of 4 mL and 20 mL of 2% lidocaine in 2 studies, were self-administered vaginally at a median of 9 and 21 minutes, respectively, prior to procedure initiation. Compared with placebo, the vaginal gels did not appear to have an impact on pain associated with IUD insertion.16,22
By contrast, an oil-in-water cream formulation containing a 1:1 lidocaine, 2.5%, and prilocaine, 2.5%, mixture (LP cream) showed promise as a pain relief strategy in a 3-armed, randomized controlled trial comparing LP cream with misoprostol (a cervical ripening agent) or placebo.23 In the LP cream group, 2 mL of the cream was applied to the ectocervix and 3 mL applied to the endocervical canal 5 minutes before IUD insertion. In the misoprostol group, a misoprostol, 200 μg, vaginal tablet was administered 3 hours before IUD insertion. Significantly lower mean (SD) VAS pain scores on a 100-mm line for both LP cream versus placebo (2.1 [1.0] vs 3.7 [1.6], respectively; P <.001) and misoprostol vaginal tablets versus placebo (2.3 [1.3] vs 3.7 [1.6]; P <.001) were noted.23 Pain control during IUD insertion with use of LP cream or misoprostol was comparable, yet use of LP cream was associated with significantly lower VAS pain scores (on a 100-mm line) at 10 minutes following the procedure compared with use of misoprostol.23 Use of LP cream also was associated with greater ease of IUD insertion and higher patient satisfaction than was use of misoprostol or placebo.23 The researchers concluded that LP cream was an effective strategy for pain control and ease of IUD insertion and that use of a misoprostol, 200 μg, vaginal tablet was a viable alternative when LP cream is unavailable.23
Use of paracervical blocks (lidocaine, 1%; 10 mL or 18 mL) has lessened pain associated with various steps of IUD insertion according to outcomes from 2 randomized clinical trials.8,24 A study evaluating the 10-mL lidocaine block involved women aged 14 to 22 years who were going to receive the 13.5-mg levonorgestrel IUD. These patients received the block 3 minutes prior to IUD insertion, with 1 mL of lidocaine, 1%, injected at the tenaculum site and 4.5 mL injected at 4 o’clock and 8 o’clock on the cervicovaginal junction.8 Another study evaluated an 18-mL lidocaine block in women aged 18 to 45 years; most were going to receive the levonorgestrel, 52-mg, IUD or the CuT380A IUD, both of which have larger applicator frames than that of the 13.5-mg levonorgestrel IUD and could influence pain experience. For the paracervical block, the 18 mL of lidocaine, 1%, was buffered with 2 mL of sodium bicarbonate, 8.4%. Patients received the 20-mL block directly before IUD insertion, with 2 mL injected at the tenaculum site and 9 mL injected at 4 o’clock and 8 o’clock on the vaginal fornices.24
In both studies, the median VAS pain score (100-mm line) for IUD insertion was lower for women given the paracervical block than for those given no block (10-mL block, 30.0 vs 71.5 mm [P < .001]; 18-mL block, 33 vs 54 mm [P =.002]).8,24 Patients who received the 10-mL lidocaine block had a lower VAS pain score (100-mm line) for every procedural step from tenaculum placement through 5 minutes after removal of the speculum.8 Similarly, patients who received the 18-mL lidocaine block had lower median pain scores for uterine sounding through 5 minutes after IUD placement.24 Of note, patients should be counseled before undergoing the procedure, as that the paracervical block itself can cause pain (30 mm on a VAS pain scale [100-mm line]), although it has effectively reduced the overall level of pain experienced with the IUD procedure.24
In summary, the findings from these studies were favorable regarding the use of certain lidocaine preparations as a local analgesic for controlling pain associated with IUD insertion.8,16,22-24
Cervical priming agents
As mentioned in the review of an earlier study, misoprostol is typically used to ripen the cervix before labor induction and transcervical procedures.23 However, according to a 2016 Centers for Disease Control and Prevention (CDC) review of studies, results of 7 of 10 trials evaluating misoprostol use in easing IUD insertion did not find a notable difference between the misoprostol and control groups. Furthermore, results from 2 trials with results favoring use of misoprostol over placebo either were confounded or showed that IUD insertions across all patients were without discomfort.25
Despite these outcomes, the CDC concluded that outcomes of 1 randomized controlled trial showed promise for misoprostol use among women who initiated a second attempt at IUD insertion after an initial failed attempt.25 Participants in the active group received misoprostol, 200 µg, vaginally either 10 hours or 4 hours before insertion; results were compared against those of a placebo group.25 With the second insertion attempt, considerably more women given misoprostol experienced a successful insertion than did those given placebo (88% vs 62%, respectively).25 The CDC noted that additional research should include focus on misoprostol use following an initial IUD insertion failure.25
Overall, misoprostol has not demonstrated efficacy in reducing pain associated with IUD insertion; however, it may support insertion success among women who experienced a previous insertion failure.24
Nitrous oxide and intrauterine analgesia
Administration of odorless and colorless nitrous oxide gas or intrauterine analgesia has been explored for IUD insertion pain; however, results are mixed, and neither strategy is widely available in the practice setting.6,11,15,26 Nitrous oxide has a strong safety profile and rapid metabolism, which allows patients to quickly assume normal activities after administration.6 One prospective observational study explored the effects of nitrous oxide versus standard of care on pain levels among adolescents following IUD placement.6 Nitrous oxide was administered via inhalation at a rate of 50/50 nitrous oxide/oxygen for 2 minutes prior to IUD insertion.6 Patient-reported pain results on a VAS pain score (100-mm line) demonstrated a lower pain experience and greater patient satisfaction with the procedure among those who used nitrous oxide than among those who received standard of care.6 Results of a 2016 study in which 50/50 nitrous oxide/oxygen was given for 2 minutes before the procedure, however, did not indicate pain reduction. Still, women who received the nitrous oxide reported greater satisfaction with their pain management than did those given placebo.26
Results are also conflicting on the use of intrauterine analgesia. Results of 1 study showed that IUD procedure pain and patient satisfaction were not different among groups given 5 mL of lidocaine, 2%, in the intrauterine cavity; naproxen, 375 mg, by mouth; or placebo 1 hour prior to the procedure.15 However, outcomes from another study regarding 10 mL of mepivacaine, 1%, or placebo placed in the intrauterine cavity showed that the treatment group experienced moderately lower pain levels as indicated on the VAS pain scale (100-mm line), although pain reduction was less than the hypothesized effect size.11
Overall, results are mixed on the use of nitrous oxide gas and intrauterine analgesia as pain control methods for IUD insertion.6,11,15,26 Furthermore, these approaches are not always available in the clinical setting and are used infrequently.
NONPHARMACOLOGIC MANAGEMENT
Nonpharmacologic options may be used for the IUD procedure with pharmacology-based pain management strategies or when pharmaceuticals are contraindicated or not available.27
Complementary approaches
Many complementary approaches address stress and anxiety, which directly affect pain perception.27 Deep, diaphragmatic breathing and/or yoga-like physical movements performed before IUD insertion can help enhance relaxation and comfort.27 Complementary therapies (eg, acupressure, aromatherapy, and soothing music) may also help reduce stress and/or pain associated with the procedure.27 Heat packs, which are often used to relieve discomfort associated with dysmenorrhea, may serve a similar purpose with gynecologic procedures, including IUD placement.27
Verbal analgesia
Verbal analgesia, in which a clinician uses low speech and a quiet tone of voice to calm the patient, also has demonstrated promise in research. In 1 study, verbal analgesia (consisting of verbal reinforcement offered during each step of the procedure with the clinician asking the patient to relax her body and reassuring that the procedure should not cause harm) was compared with use of tramadol hydrochloride, 50 mg, given orally 1 hour before IUD insertion. No notable differences between the 2 groups regarding overall pain level, ease of insertion, and number of insertion attempts were found.28
Atraumatic forceps
Different forceps have also been investigated for associations with pain level during IUD insertion. The single-toothed tenaculum, which pierces the cervical epithelium, was believed to cause more pain and bleeding than relatively atraumatic forceps such as the Allis or Littlewood forceps.14 However, study findings demonstrated no significant pain difference between the 2 types of forceps at the time of forceps application or IUD insertion and 5 minutes following IUD insertion.14
Timing with menstrual cycle
The World Health Organization guidelines state that IUDs may be inserted at any time throughout the menstrual cycle. Placing an IUD during menstruation may offer greater ease of insertion and less pain, because the cervical ostium is dilated; moreover, it may result in less prolonged bleeding, because the endometrium is in the process of breaking down. The challenge involved is that women are less likely to want to receive the procedure during menstruation.29 Furthermore, results from a randomized trial comparing the IUD insertion experience in women who were menstruating to those who were not menstruating showed no difference between the groups regarding pain perception at time of insertion or bleeding pattern and patient satisfaction at 3 months.29 The researchers concluded that the IUD could be inserted at any point throughout the menstrual cycle without compromising patient comfort or outcomes.29
In conclusion, nonpharmacologic options—such as deep breathing, heat packs, or verbal analgesia—may help either to complement pharmacology-based pain management or to offer relief when pharmaceuticals are not used with the IUD procedure.27,28
ACKNOWLEDGING THE PATIENT EXPERIENCE
The advent of social media platforms has offered patients valuable forums for sharing and receiving information regarding health care and the patient experience; with the expanding availability of mobile devices, these forums can be accessed by an ever-increasing majority of people.30 Most Americans now use the internet to search for health-related information that may affect their medical decision-making.30 Stories reflecting patient experience, particularly when they generate emotion from the viewer, can have a strong impact.30 Overall, social media can amplify the more-extreme patient experiences.30
Recently, social media trends regarding patient experience with IUD insertion were exposed.31-33 Findings from an evaluation conducted by Duke University indicated that 39.8% of 100 top-liked videos tagged #IUD on the social media platform TikTok highlighted a negative user experience with IUDs. In addition, 96.8% of 31 videos regarding experience with IUD insertion or removal emphasized pain and IUD adverse effects, and approximately 25% indicated patient interest in receiving anesthesia during insertion.33 Messages shared by patients via TikTok described the pain of insertion (eg, the “worst pain imaginable”) and questioned the lack of pain management options offered by the provider.31 This movement on social media highlights the need for providers to be aware of the patient experience, to address any discrepancy between provider and patient perception of pain, and to offer a viable pain management strategy for the IUD procedure.
CONCLUSIONS
IUD placement is associated with a high rate of efficacy, length of continuation, and patient satisfaction with insertion.2 The high efficacy seen in clinical practice is supported by clinical trial outcomes.2 However, anticipated insertion pain may contribute to low use despite the availability of multiple ways to manage and address insertion pain.2,6 Various approaches to management of associated pain have been explored. Some strategies (eg, use of certain lidocaine formulations and delivery systems) have demonstrated efficacy, although no single standard treatment algorithm has been created or described.16,19
There is an ongoing need to improve upon approaches for IUD insertion pain management.19 Health care providers tend to underestimate pain, and they need to recognize that the pain of IUD placement is a real barrier that must be addressed openly and effectively.12 Determining each patient’s potential pain threshold and susceptibility to discomfort may help guide an individualized analgesic plan.18,19 Thoughtful conversations can increase patient comfort when they receive an IUD. Improved pain management may also allow the provider to insert the device more smoothly and quickly, and it may help patients feel greater satisfaction with the procedure.23 Ultimately, it would address a barrier to IUD use and subsequently increase IUD usage and decrease unintended pregnancies.34
REFERENCES
1. Finer LB, Zolna MR. Declines in unintended pregnancy in the United States, 2008-2011. N Engl J Med. 2016;374(9):843-852. doi:10.1056/NEJMsa1506575
2. de Oliveira ECF, Baêta T, Brant APC, Silva-Filho A, Rocha ALL. Use of naproxen versus intracervical block for pain control during the 52-mg levonorgestrel-releasing intrauterine system insertion in young women: a multivariate analysis of a randomized controlled trial. BMC Womens Health. 2021;21(1):377. doi:10.1186/ s12905-021-01521-z
3. Abu-Zaid A, Alshahrani MS, Albezrah NA, et al. Vaginal dinoprostone versus placebo for pain relief during intrauterine device insertion: a systematic review and meta-analysis of randomised controlled trials. Eur J Contracept Reprod Health Care. 2021;26(5):357-366. doi:10.1080/13625187.2021.1891411
4. IUDs and implants: LARC—long acting reversible contraception. North American Society for Pediatric and Adolescent Gynecology. Revised October 2020. Accessed January 23, 2024. https://www. naspag.org/assets/docs/larc_2020.pdf
5. Hardeman J, Weiss BD. Intrauterine devices: an update. Am Fam Physician. 2014;89(6):445-450.
6. Fowler KG, Byraiah G, Burt C, Lee DB, Miller RJ. Nitrous oxide use for intrauterine system placement in adolescents. J Pediatr Adolesc Gynecol. 2022;35(2):159-164. doi:10.1016/j.jpag.2021.10.019
7. Trussell J. Contraceptive failure in the United States. Contraception. 2011;83(5):397-404. doi:10.1016/j. contraception.2011.01.021
8. Akers AY, Steinway C, Sonalkar S, et al. Reducing pain during intrauterine device insertion: a randomized controlled trial in adolescents and young women. Obstet Gynecol. 2017;130(4):795- 802. doi:10.1097/AOG.0000000000002242
9. Daniels K, Abma JC. Current contraceptive status among women aged 15-49: United States, 2017-2019. Centers for Disease Control and Prevention. Reviewed October 20, 2020. Accessed January 23, 2024. https://www.cdc.gov/nchs/products/databriefs/db388.htm
10. Alotaibi M, Aljahany M, Alhamdan Z, Alsaffar M, Almojally A, Alassaf W. Differences in acute pain perception between patients and physicians in the emergency department. Heliyon. 2022;8(11):e11462. doi:10.1016/j.heliyon.2022.e11462
11. Envall N, Lagercrantz HG, Sunesson J, Kopp Kallner H. Intrauterine mepivacaine instillation for pain relief during intrauterine device insertion in nulliparous women: a double-blind, randomized, controlled trial. Contraception. 2019;99(6):335-339. doi:10.1016/j.contraception.2019.02.003
12. Akintomide H, Brima N, Sewell RDE, Stephenson JM. Patients’ experiences and providers’ observations on pain during intrauterine device insertion. Eur J Contracept Reprod Health Care. 2015;20(4):319-326. doi:10.3109/13625187.2015.1031885
13. Ngo LL, Braaten KP, Eichen E, Fortin J, Maurer R, Goldberg AB. Naproxen sodium for pain control with intrauterine device insertion: a randomized controlled trial. Obstet Gynecol. 2016;128(6):1306-1313. doi:10.1097/AOG.0000000000001746
14. Speedie JMM, Mansour D, Landy R, Clement KM. A randomised trial comparing pain and ease of use of two different stabilising forceps for insertion of intrauterine contraception. J Fam Plann Reprod Health Care. 2016;42(4):241-246. doi:10.1136/ jfprhc-2016-101446
15. Miles SM, Shvartsman K, Dunlow S. Intrauterine lidocaine and naproxen for analgesia during intrauterine device insertion: randomized controlled trial. Contracept Reprod Med. 2019;4:13. doi:10.1186/s40834-019-0094-0
16. Conti JA, Lerma K, Schneyer RJ, Hastings CV, Blumenthal PD, Shaw KA. Self-administered vaginal lidocaine gel for pain management with intrauterine device insertion: a blinded, randomized controlled trial. Am J Obstet Gynecol. 2019;220(2):177. e1-177.e7. doi:10.1016/j.ajog.2018.11.1085
17. De Nadai MN, Poli-Neto OB, Franceschini SA, et al. Intracervical block for levonorgestrel-releasing intrauterine system placement among nulligravid women: a randomized double-blind controlled trial. Am J Obstet Gynecol. 2020;222(3):245.e1-245.e10. doi:10.1016/j.ajog.2019.09.013
18. Perez-Lopez FR, Martinez-Dominguez SJ, Perez-Roncero GR, Hernandez AV. Uterine or paracervical lidocaine application for pain control during intrauterine contraceptive device insertion: a meta-analysis of randomised controlled trials. Eur J Contracept Reprod Health Care. 2018;23(3):207-217. doi:10.1080/1362 5187.2018.1469124
19. Gemzell-Danielsson K, Jensen JT, Monteiro I, et al. Interventions for the prevention of pain associated with the placement of intrauterine contraceptives: an updated review. Acta Obstet Gynecol Scand. 2019;98(12):1500-1513. doi:10.1111/aogs.13662
20. Lopez LM, Bernholc A, Zeng Y, et al. Interventions for pain with intrauterine device insertion. Cochrane Database Syst Rev. 2015;2015(7):CD007373. doi:10.1002/14651858.CD007373.pub3
21. Crawford M, Davy S, Book N, Elliott JO, Arora A. Oral ketorolac for pain relief during intrauterine device insertion: a double-blinded randomized controlled trial. J Obstet Gynaecol Can. 2017;39(12):1143-1149. doi:10.1016/j.jogc.2017.05.014
22. Rapkin RB, Achilles SL, Schwarz EB, et al. Self-administered lidocaine gel for intrauterine device insertion in nulliparous women: a randomized controlled trial. Obstet Gynecol. 2016;128(3):621-628. doi:10.1097/AOG.0000000000001596
23. Hashem AT, Mahmoud M, Aly Islam B, et al. Comparative efficacy of lidocaine-prilocaine cream and vaginal misoprostol in reducing pain during levonorgestrel intrauterine device insertion in women delivered only by cesarean delivery: a randomized controlled trial. Int J Gynaecol Obstet. 2022. doi:10.1002/ijgo.14157
24. Mody SK, Farala JP, Jimenez B, Nishikawa M, Ngo LL. Paracervical block for intrauterine device placement among nulliparous women: a randomized controlled trial. Obstet Gynecol. 2018;132(3):575-582. doi:10.1097/AOG.0000000000002790
25. Zapata LB, Jatlaoui TC, Marchbanks PA, Curtis KM. Medications to ease intrauterine device insertion: a systematic review. Contraception. 2016;94(6):739-759. doi:10.1016/j. contraception.2016.06.014
26. Singh RH, Thaxton L, Carr S, Leeman L, Schneider E, Espey E. A randomized controlled trial of nitrous oxide for intrauterine device insertion in nulliparous women. Int J Gynaecol Obstet. 2016;135(2):145-148. doi:10.1016/j.ijgo.2016.04.014
27. Passmore RC, Gold MA. Nonpharmacologic approaches to pain management with IUD insertion. In: Coles M, Mays A, eds. Optimizing IUD Delivery for Adolescents and Young Adults. Springer; 2019:123-132. doi:10.1007/978-3-030-17816-1_10
28. Daykan Y, Battino S, Arbib N, et al. Verbal analgesia is as good as oral tramadol prior to intrauterine device (IUD) insertion, among nulliparous women: a randomized controlled trial. Eur J Obstet Gynecol Reprod Biol. 2021;258:443-446. doi:10.1016/j. ejogrb.2020.09.019
29. van der Heijden P, Geomini P, Herman MC, Veersema S, Bongers MY. Timing of insertion of levonorgestrel-releasing intrauterine system: a randomised controlled trial. BJOG. 2017;124(2):299-305. doi:10.1111/1471-0528.14445
30. Patrick M, Venkatesh RD, Stukus DR. Social media and its impact on health care. Ann Allergy Asthma Immunol. 2022;128(2):139-145. doi:10.1016/j.anai.2021.09.014
31. Sung M. Viral TikToks about IUDs portray distrust of doctors, new research shows. NBC News. December 16, 2022. Accessed February 13, 2024. https://www.nbcnews.com/health/ sexual-health/iud-tiktok-study-duke-university-distrust-healthcare-misinformation-rcna61769
32. IUDs are highly effective, but some women find insertion painful. New York Times Facebook page. July 3, 2022. Accessed February 13, 2024. https://m.facebook.com/nytimes/ posts/10152955614484999/
33. Wu J, Trahair E, Happ M, Swartz J. TikTok, #IUD, and user experience with intrauterine devices reported on social media. Obstet Gynecol. 2023;141(1):215-217. doi:10.1097/ AOG.0000000000005027
34. Samy A, Ali AS, Latif D, Darweesh FF, Ghamry NK, Metwally AA. Benefits of self-administered vaginal dinoprostone 12 hours before levonorgestrel-releasing intrauterine device insertion in nulliparous adolescents and young women: a randomized controlled trial. J Pediatr Adolesc Gynecol. 2020;33(4):382-387. doi:10.1016/j.jpag.2020.02.01
Read the full issue here.












Severe maternal morbidity linked to mental health risks post-delivery
April 26th 2024A recent study revealed that severe maternal morbidity during pregnancy increases the likelihood of mental health hospitalizations or emergency department visits up to 13 years post-delivery, emphasizing the need for mental health screening.
Read More


FDA approves updated label for Biktarvy against HIV-1
April 26th 2024Gilead Sciences has announced FDA approval of an updated Biktarvy label, showcasing safety and efficacy data from a phase 1b trial, positioning it as a pivotal treatment option for pregnant individuals with HIV-1 and suppressed viral load.
Read More

No link found between antenatal corticosteroids and child neurodevelopment
April 25th 2024A recent study found no link between antenatal corticosteroid administration and adverse neurodevelopmental outcomes in children aged 6 years or older, offering reassurance for late preterm delivery practices.
Read More


