Analysis of the longest running ICSI programme in the United States has found reassuring evidence that babies born from frozen embryos fertilised via ICSI (intracytoplasmic sperm injection) do just as well as those born from frozen embryos fertilised via standard IVF treatment.
OBGYN.net Staff
Advertisement
Articles by OBGYN.net Staff
Researchers have found evidence that chronic disease in either a mother or father can create unfavourable conditions in the womb that are associated with the development of polycystic ovarian syndrome (PCOS) in daughters.
Until now there has been no evidence-based consensus amongst fertility specialists as to whether or not men should refrain from sex for a few days before attempting to conceive with their partner, either spontaneously or via assisted reproduction.
Comments from Specialists I heard from a reliable newspaper or television station that he implanted 6 and two of the embryos split into twins. Allen Worrall, RDMS Intra - endometrial implantation is evolving to be a superior method and Dr Kamrava deserves recognition for this contribution but......if hysteroscopic embryo implantation is supposed to be 70% more effective than the "blind technique", why then would Dr Kamrava aim to obtain 8 pregnancies??????George Haber, MD Regardless of the media hype and not knowing the inside story of why so many embryos were implanted, we have apparently a high success rate technique with zero ectopics, this is worth considering. Let's separate science from entertainment.Mario E. Domenzain, M.D., F.A.C.O.G. What we so far know about implantation is that it is a very complex process, where a sequence of events happens with a very delicate synchronization (selection of the site of implantation by Selectin molecules which help the blastocyst "roll" to the right spot, MUC-1 repelling it from the "bad" ones, chemokines and cytokines -LIF, IL-1. Integrins- attracting it, adhesion molecules attaching it to pinopodes, to cite a few). I doubt that forcibly "implanting" an embryo into a self-selected spot in the endometrium could really improve pregnancy rates; it is bypassing the natural selection process (for example: embryos do not "take" on endometrium without pinopodes either because of poor timing or because of endometrium defect). Hysteroscopic embryo implantation might reduce the rate for ectopic pregnancies. But unless the hysteroscopic process in itself stimulates the release of these molecules on the spot (like the repeated Pipelle might be doing???), it should not improve the overall pregnancy rate. I of course -and all my IVF team in Jerusalem, where we do see several very religious women "pushing" for many children!!!, cannot agree with replacing 8 embryos by ANY type of woman (especially if she is young and proven fertile !!!!) Dr Hava-Yael Schreiber, M.DOB/GYN and Fertility specialist Zir Chemed Medical Center and Bikur Holim Hospital, Jerusalem Roberta and friends, There has been such a media frenzy about this, and for good reason. While any licensed practitioner is theoretically entitled to their own opinion about procedures, standard of care dictates the concept of evidence-based medicine, i.e. do no harm and do what is reasonable based on the best interpretation of peer-reviewed medical literature. When Dr. Kavarna gave this interview awhile ago, perhaps he had a hypothesis that hysteroscopic assistance of embryo transfers would aid the success of implantation. To my knowledge, he hasn't proven the value of this technique, nor has anyone else. And in fact, the standard of care has become ultrasound-assisted embryo transfer, which is hardly a blind technique. In fact, many centers (such as ours) utilize echo-tip catheters which allow for excellent visualization of transfer catheter placement via abdominal ultrasound, especially when the patient has a moderately full bladder. Now as far as results, prospective patients who are looking into IVF, along with their physicians, should be strongly urged to evaluate data published annually online by the Society for Assisted Reproductive Technology (SART) at www.sart.org Although there is a lag in SART's ability to compile and post data, both patients and physicians can get an idea of who is doing what, practice-by-practice, and both nationally and regionally. Currently, the latest data listed on the SART website is from 2006, but I believe 2007 will be available soon. Most SART clinics have already compiled preliminary 2008 data but have not yet submitted, mainly because final results are not in yet for live births generated from 2008 cycles. Now, you asked about our data. And here is what I can share, which is available already publicly (2006) and will soon be available publicly (2007): For women under 35 using fresh non-donor eggs, the live birth rate per transfer in 2006 was 51.4 percent, and we transferred an average of 1.8 embryos for those patients. For that group, 22.2 percent had elective single embryo transfer. The overall implantation rate was 43.1% (see https://www.sartcorsonline.com/rptCSR_PublicMultYear.aspx?ClinicPKID=2442 for the full summary) In 2007 for the same group, the live birth rate per transfer was 55.1%, and we transferred an average of 1.4 embryos. Approximately 60% of our patients < 35 had a single embryo transfer. SART calculates the implantation rate after the data is submitted, but I would estimate it to be around 45-50%. This trend towards "fewer is better" is again seen in our preliminary 2008 results. We had an abstract at ASRM in 2007 which also concluded this, based on the results we had at that time. There is so much focus these days on clinics that are doing a substandard job, I think it's time for the media to infuse some hope into those who could benefit from great fertility care, and by letting people know there are some centers that are exceeding national averages and have the data to prove it. There are many important factors that go into generating high success rates, and I'm happy to discuss this further with anyone in the media who might be interested. Regards to all,Ronald F. Feinberg MD, PhDIVF Medical Director Reproductive Associates of Delaware Suite 3217, Medical Arts Pavilion 2 4735 Ogletown-Stanton Road Newark, DE 19713 302-623-4242 FAX 302-623-4241www.ivf-de.org "The ethical, personal care that helps families grow." Dear Editor of Ob-Gyn Net: I was appalled and saddened when I heard that a physician had intentionally transferred multiple embryos into a woman who had already had a multiples birth. This showed very poor judgment, in my opinion. It is also contrary to the guidelines of SART for infertility clinics. Because of all of the potential problems for these ultra-light babies, now and in the future, it is against the ethical principle of justice or “community good”. I am sure the California Board of Medical Examiners will be looking into this and well they should. The public is rightly infuriated over this situation and should demand an investigation by the Board if it is not forthcoming. Even the old caution that doctors have tried to follow for centuries, “primum non-nocere”, first, do no harm, has been breached. This whole situation likely will result in new laws or requirements for REIs and clinics that specialize in infertility. Thomas F. Purdon, MD FACOG No need to apologize. Many of us were curious about this individual, and you gave us what you had. I didn't see it as flashy or trashy--it was a legitimate interview about a relevant topic. Remember, curious people want to know.Steven Nelson MDPhoenix, AZ Dear Madam: Greetings! The interview was done as if we are condoning this procedure. Maybe this is becoming a moral issue like doctors playing God. Yes the interview was done in poor taste the interviewer allowing himself to be manipulated. Thank you and more power.Dr. Ferry AnolinManila, Phillipines I think it sounds like a very innovative procedure that may improve outcomes. (Obviously using only 1 or 2 embryos) Ginger H. Riley
Stillbirth rate is an important indicator of access to and quality of antenatal and delivery care. Obtaining overall estimates across various regions of the world is not straightforward due to variation in definitions, data collection methods and reporting.
Intrauterine infection is considered as one of the major maternal insults during pregnancy. Intrauterine infection during pregnancy could lead to brain damage of the developmental fetus and offspring.
A substantial number of European patients travel to other countries for fertility treatment, both because they think that they will receive better quality care abroad and in order to undergo procedures that are banned in their home country says a study of the subject launched at the 25th annual conference of the European Society of Human Reproduction and Embryology today (Monday June 29).
In February 1988, the patient, a 26-year-old married woman, experienced moderate vaginal bleeding. She contacted her gynecologist, who referred her to an ultrasound clinic for a sonographic workup.
Although the incidence of shoulder dystocia is low (reported between 0.6% and 1.4%), it continues to be a clinical challenge for birth attendants and is among the 4 largest causes of monetary awards in obstetric tort cases.
This case study presents a 35-year-old white female who was referred to the UAMS High-Risk Obstetrical Clinic due to advanced maternal age. The patient and her husband received genetic counseling. This was the patient's first pregnancy. She presented with no obvious complications.
The diagnosis of trisomy 21 was made by chorion villus sampling because of increased (3,2 mm) fetal nuchal translucency thickness detected at routine first-trimester ultrasonographic examination.
To study the value of Doppler ultrasound of the ductus venosus in the screening for chromosomal abnormalities at 10-14 weeks of gestation.
The mobile foraminal flap consisted of a thin membrane ballooning into the left atrium. During ventricular filling, the flap encroached on the mitral valve annulus, but did not appear to obstruct the mitral valve flow.
Twin to twin transfusion syndrome (TTTS) is a common complication of monochorionic twin gestations. If untreated, this condition carries a very high mortality rate for both twins. The therapeutic options available today are still rather limited.
Over the past 10 years controversy has surrounded the practice of ultrasound for entertainment purposes. In 1994, the ARDMS held and published a readership poll on this very subject. For our paper we decided to hold a similar poll to see if the opinion has changed over the last 5 years.
Hypoplasia of the right ventricle is uncommon as an isolated entity. It may result from tricuspid atresia, but is most commonly secondary to pulmonary atresia with intact ventricular septum.
Gynecology Images: Normal Abnormal Obstetric Images: 1st Trimester: Normal Abnormal 2nd Trimester: Normal Abnormal 3rd Trimester: Normal Abnormal Medical Professionals: Upload Your Here Obstetric Images: 3rd Trimester: Normal Normal Thymus - Albana Cerekja Fetal urethra at 31 weeks: just before micturition - Albana Cerekja Normal Female: 4D still image - Effendi Mansoor Monolateral double renal artery,: Normal variant kidney artery supply - Albana Cerekja TRV Fetal Head: BPD and HC Measurements - SIEMENS Velamentosa insertion: 3rd trimester - Effendi Mansoor Umbilical Cord (3D Surface Rendering): Normal Cord - MEDISON SAG Fetal Face, Profile: Fetal Breathing on Color Doppler - SIEMENS 3D Surface Reconstruction: Face - Cayrol Guillermo 3D Surface Reconstruction: Extended Breech Presentation - Saied Mohamed Tohamy 3D Surface Reconstruction: Face - Juan Carlos Pons 3D Surface Reconstruction: Face and Foot - Cayrol Guillermo 3D Surface Reconstruction: Face - Juan Carlos Pons 3D Surface Reconstruction: Face - Juan Carlos Pons
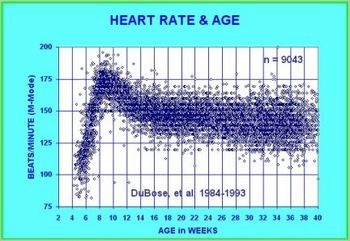
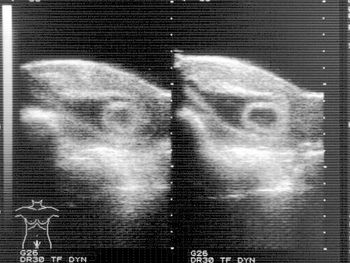
The embryonic heart rate (EHR) has been found to correlate with gestational age by crown-rump length (CRL) in normal pregnancies. This research compares the EHR and CRL for a population (n=173) in an assisted fertility program, and a population (n=173) of normal pregnancies which were paired by CRLs.
There are many factors that go into the decision to choose a birth control method. This article is intended to be an overview to help you to think about these choices, and make a decision about what method is best for you.
(fig. 1) I was so astonished by the 3D image that I wanted to share with you. Look at the shape of the copper coil, it's amazing. Submitted by Daniel Margulies, Argentina. (fig. 2) "This is my best 3D Multiplanar Reconstruction of Multiload IUD."Image provided by:Mrio Libardi, M.D.Multimagem Ultra-sonografiaBotucatu, Sao PauloBrasil (fig. 3) Image provided courtesy of Antwoord van dr. R.J.C.M. Beerthuizen, directeur Stichting Anticonceptie Nederland, Winterswijk (fig. 4) Image provided by:Mrio Libardi, M.D.Multimagem Ultra-sonografiaBotucatu, Sao PauloBrasilFor more images and information about IUDs, please click here CommentsMy gut tells me that this may be an image artifact that is unique to 3D sonography. If any of you heard the lecture on 3D artifacts in Buenos Aries by Dr. Andrew Hull... he was clear that 3D introduces new categories of image artifacts and a new "twist" on old familiar artifacts. You can see the interview of Dr. Hull at:http://www.obgyn.net/displaytranscript.asp?page=/avtranscripts/dubose_hull This is probably not useful pathologically, but as a phenomenon of 3D sonography it may be important educationally to us end users. I would like to post it and see more discussion. Peace, Terry J. DuBose, M.S., RDMS Assistant Professor & Director, Diagnostic Medical Sonography Program CHRP, University of Arkansas for Medical Sciences Little Rock, Arkansas, USA 501-686-6510http://www.io.com/~dubose/http://www.uams.edu/CHRP/dmshome.htmhttp://www.obgyn.net/us/panel/panel.htm
The contraceptive patch (Ortho Evra™ transdermal system) is a weekly hormonal birth control method that received Food and Drug Administration approval in November 2001. The product is an adhesive patch, similar to a large Band Aid®, that a woman places onto her skin to prevent pregnancy. The patch contains hormones that are released through the skin and into the bloodstream.
The purpose of the Women’s Health Initiative hormone program was to study the health benefits and risks of hormones for postmenopausal women. In July 2002, we asked women in the estrogen plus progestin part of the program to stop taking their study pills.
Recent research by members of the Population Council's International Committee for Contraception Research (ICCR) and other scientists shows that emergency contraceptive pills appear to work by interfering with ovulation, thus preventing fertilization of the egg.
Advertisement
Advertisement
Advertisement
Trending on Contemporary OB/GYN
1
FDA: Levonorgestrel/ethinyl estradiol birth control patch sees update to labeled strength
2
Using a self-collected vaginal fluid test for endometrial cancer detection
3
Quynh Tran, MD, explains the state of sexual medicine education in the Midwest
4
Shared decision-making key to non-hormonal VMS and sleep management in menopause
5